Is Dry FIP More Difficult to Treat Than Wet FIP

Feline Infectious Peritonitis (FIP) is one of the most challenging diseases in feline medicine, perplexing veterinarians and devastating cat owners worldwide. It develops as a result of a mutation in the feline coronavirus (FCoV), transforming a typically benign infection into a progressive and usually fatal illness. The disease manifests in two primary forms: the effusive or "wet" form, and the non-effusive or "dry" form. Understanding whether dry FIP is actually more difficult to treat than wet FIP requires a deep dive into their biological, clinical, and therapeutic differences.
FIP Fundamentals: Mutation & Immunopathology
FIP arises when a common, often harmless feline enteric coronavirus mutates within a cat’s body. This mutated virus acquires the ability to replicate within macrophages, leading to an uncontrolled, widespread inflammatory response. The result is vasculitis, granuloma formation, and multi-organ impairment—hallmarks of FIP. The cat’s immune system plays a paradoxical role, simultaneously attempting to contain the virus but also contributing to tissue damage. The unique immunopathology underlying dry versus wet FIP shapes both the presentation and therapeutic response.
The Wet Form: Effusive Presentation and Diagnosis
Wet FIP is characterized by the abnormal accumulation of fluid in body cavities—most commonly the abdomen (ascites) and chest (pleural effusion). This form typically leads to rapid clinical deterioration, with the cat displaying symptoms such as lethargy, weight loss, and severe breathing difficulties. The abundance of protein-rich fluid often allows veterinarians to make a clinical diagnosis with relative confidence, supported by laboratory findings such as elevated globulins and low albumin.
The rapid progression of wet FIP paradoxically offers two advantages in detection and management: First, classic symptoms prompt owners to seek veterinary care sooner, increasing the likelihood of diagnosis during an earlier phase of disease. Second, the ability to sample effusion fluid can provide high-yield specimens for testing, including cytology and PCR, frequently leading to swift confirmation.
The Dry Form: Non-Effusive Challenge and Diagnostic Hurdles
Dry FIP, in contrast, presents with granulomatous inflammation rather than fluid effusion. Organ involvement varies, including the liver, kidneys, lymph nodes, eyes (ocular FIP), and the central nervous system (neurological FIP). Neurological and ocular variants are especially insidious, often eluding diagnosis for weeks or months as symptoms mimic other diseases. Clinical signs are usually non-specific: chronic fever, weight loss, behavioral changes, ocular lesions, or neurological deficits.
Because no effusion is present, ante-mortem diagnosis is challenging. Veterinarians rely more on indirect evidence, such as hyperglobulinemia, persistent fever, lymphopenia, and serology or PCR. Conclusive diagnosis sometimes requires invasive biopsies, which carry risks in debilitated cats. Consequently, many cases of dry FIP are only confirmed post-mortem, or when empirical treatment yields dramatic improvement.
Therapeutic Landscape: GS-441524, Remdesivir, and Novel Therapies
As of the mid-2020s, breakthroughs have transformed FIP from a uniformly fatal disease to one with hope. Nucleoside analogues, especially GS-441524 and its prodrug remdesivir, demonstrated potent antiviral activity in controlled studies and field treatments. Both drugs target the viral replication machinery, rapidly reducing viral load and mitigating the pathogenic immune response.
Treatment protocols for FIP depend on several variables, including form (wet vs dry), severity, and organ involvement. Wet FIP, due to its classic presentation and generally systemic distribution, often responds well to 12–14 weeks of antiviral therapy. Many cats achieve remission and long-term survival if therapy is initiated early and compliance maintained.
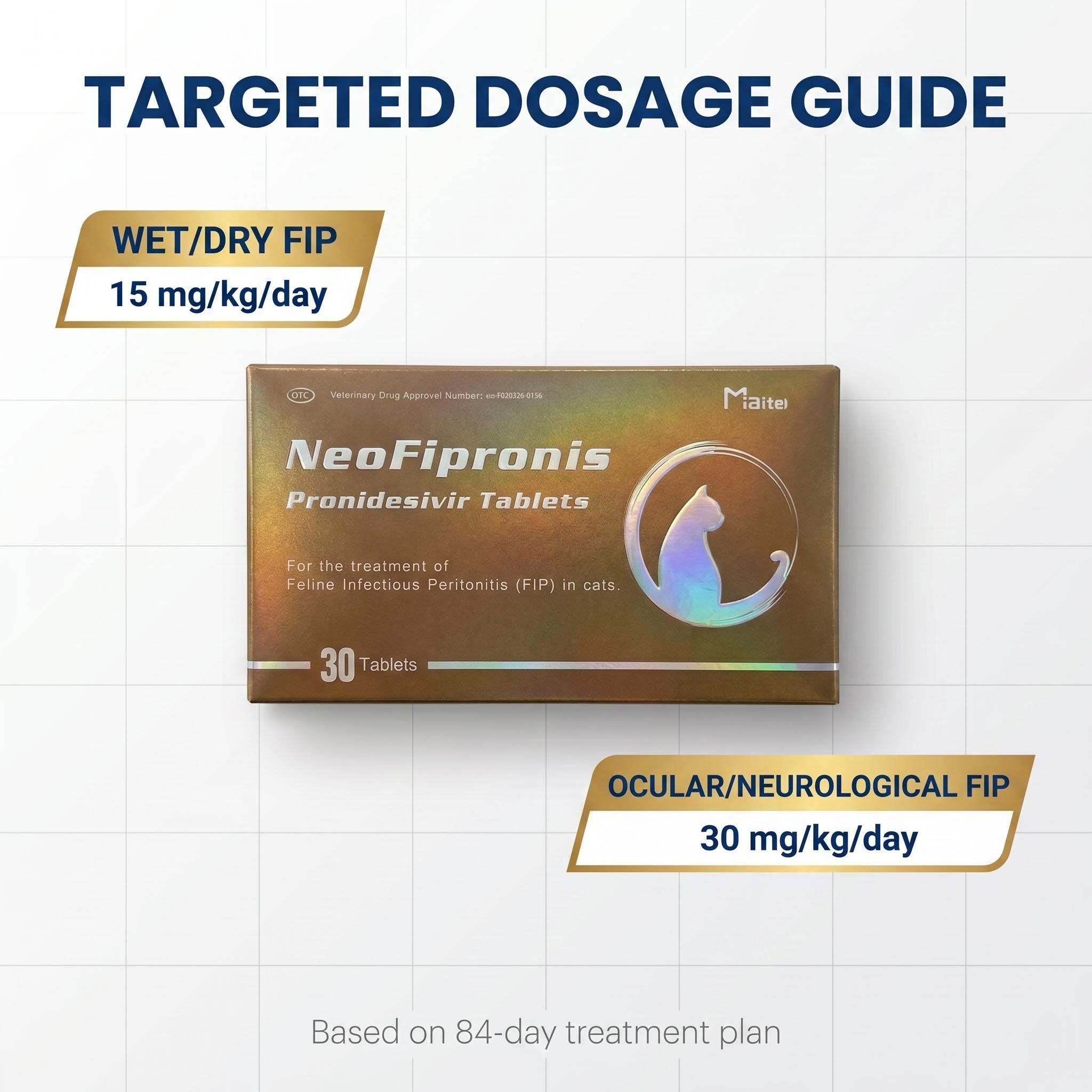
Dry FIP, by contrast, introduces several complexities. Neurological and ocular involvement require higher drug dosages due to blood-brain and blood-ocular barriers, and clinical response is slower. Cats with CNS FIP often need double or triple the standard dose of GS-441524 to achieve adequate cerebrospinal fluid penetration. The prolonged course also raises costs and logistical challenges, as frequent neurological evaluations and imaging may be necessary.
Prognosis: Survival Rates and Relapse Risk
Published studies and anecdotal reports show clear trends: Cats with wet FIP generally have better survival rates when treated with antivirals, approaching 80–90% remission in some studies. Dry FIP, especially with CNS or ocular involvement, has a lower success rate, hovering around 55–75% depending on treatment timing and drug penetration. Relapses also occur more frequently in dry FIP, with some cats requiring re-treatment cycles or combination therapies.
The difference in prognosis reflects, in part, the insidious nature of dry FIP. Because dry FIP may evolve slowly, cats present later in disease course, often with advanced granulomatous lesions. These lesions are difficult to reverse, even with effective antivirals, and systemic recovery may be incomplete.
Supportive Care Challenges: Managing Complications
Both wet and dry FIP cases require comprehensive supportive care, but dry FIP more often necessitates multi-disciplinary management. Cats with neurological involvement may require anticonvulsants, corticosteroids to reduce inflammation, physical rehabilitation, and nutritional support. Ocular FIP cases call for topical agents, periodic ophthalmological evaluation, and possible surgical intervention for complications like glaucoma or uveitis. Involvement of organs such as the liver or kidneys introduces the need for anti-nausea drugs, fluid therapy, and monitoring for organ failure.
Wet FIP cases, on the other hand, center around managing effusions—drainage may be needed for comfort, but most improvement comes from antiviral therapy as fluid production wanes. Because effusive FIP shows a dramatic clinical response to treatment, supportive care is often less prolonged and complex.
Diagnostic Advances: Immunohistochemistry, PCR, and AI-Based Tools
Technological improvement in FIP diagnostics has begun to narrow the gap in detection, especially important for dry FIP. Immunohistochemistry of biopsied tissues, quantitative RT-PCR, and new AI-based risk scoring tools improve early identification. However, limitations remain: PCR cannot distinguish between benign and pathogenic FCoV strains in the absence of clinical context. The cost and accessibility of advanced diagnostics also challenge community-based practice.
Routine laboratory markers, such as the albumin-to-globulin ratio, continue to aid in presumptive diagnosis—but their specificity is reduced in dry FIP, as overlapping conditions (lymphoma, chronic infectious disease) can produce similar patterns. Thus, a combination of clinical suspicion, advanced imaging, and molecular testing is required for dry FIP, rendering it both costlier and more elusive.
Immunological Insights: Monoclonal Antibodies and Adjunctive Therapy
Emerging therapies targeting the cat's immune dysregulation are under investigation. Monoclonal antibodies, anti-inflammatory agents, and immune modulators like polyprenyl immunostimulant have entered pilot studies, with varying degrees of efficacy. These treatments show promise particularly in chronic dry FIP, where granulomatous inflammation persists despite viral reduction. Adjunctive therapy may enhance recovery or prevent relapse but requires further research to define their role.
Access and Owner Experience: Navigating Treatment Journeys
From an owner’s perspective, dry FIP is harder to detect, treat, and monitor. Delayed diagnosis, lengthy therapy, and increased risk of relapse strain both emotional and financial resources. Many owners must coordinate visits to specialty clinics for advanced imaging or neurological evaluation. Additionally, some legal and regulatory frameworks limit access to first-line antivirals, complicating the logistics of care.
Support groups and educational resources have emerged to guide owners through the intricacies of dry FIP management. Online communities, telemedicine consults, and crowd-sourced funding all play roles in expanding treatment access, but disparities persist. Veterinary professionals emphasize early intervention, strict compliance, and multidisciplinary teamwork, especially for cats with dry FIP.
Preventative Strategies: Limiting FCoV Exposure and Management
Reducing FIP incidence remains a major focus. Best practices include minimizing overcrowding in multi-cat households, maintaining rigorous cleaning protocols, and isolating cats showing signs of illness. Breeders, shelters, and veterinarians work to reduce FCoV transmission—recognizing that not all cats exposed will develop FIP, but controlling the spread of the virus lessens overall risk.
No vaccine currently exists with proven efficacy against FIP, although research continues. Early screening of breeding cats for chronic FCoV shedding may curb transmission—and some novel biotherapeutic approaches aim to block viral entry into macrophages, providing preventive value especially in high-risk populations.
Ongoing Research: New Horizons in FIP Treatment
The landscape of FIP management continues to evolve, with clinical trials underway for next-generation antivirals, combination therapies, and gene-editing candidates. Improved formulation of GS-441524 for oral administration could enable at-home therapy, especially for dry FIP cases requiring long courses. Targeted drugs designed for blood-brain barrier penetration may revolutionize CNS FIP treatment, and better longitudinal studies clarify relapse risk and optimal dosing regimens.
Advances in diagnostics, including point-of-care biomarker tests and improved imaging modalities, may allow earlier intervention. Artificial intelligence tools and telemedicine platforms support continuous monitoring and tailored care plans—a boon for cats with chronic or atypical disease. As research advances, consensus around the complexities of treating dry versus wet FIP continues to sharpen.
Why Dry FIP Challenges Treatment More Than Wet FIP
Dry FIP’s complexity lies in its subtle presentation, multi-organ involvement, and frequent progression to neurological or ocular disease. Diagnosis is often delayed or requires invasive procedures, treatment protocols are more aggressive and prolonged, and owner burden is higher. Clinical response is slower, and relapse rates remain significant compared to wet FIP.
Effusive FIP, while severe, allows earlier detection and typically responds rapidly to available antivirals, provided therapy starts before irreversible organ damage. Thus, among veterinarians and researchers, consensus is growing: dry FIP, particularly with nervous system involvement, is indeed more difficult to treat effectively than wet FIP.
References
1. Pedersen, N.C., et al. "Efficacy and Safety of the Nucleoside Analogue GS-441524 for Treatment of Cats with Naturally Occurring Feline Infectious Peritonitis." Journal of Feline Medicine and Surgery, vol. 21, no. 4, 2019, pp. 271–281.
2. Krentz, D., et al. "Clinical diagnosis and management of feline infectious peritonitis." Veterinary Clinics: Small Animal Practice, vol. 47, no. 3, 2017, pp. 721–746.
3. Felten, S., et al. "Feline infectious peritonitis—A review of pathogenesis, diagnostics, and novel therapeutics." Veterinary Journal, vol. 254, 2019, pp. 17–23.
4. Dewerchin, H.L., et al. "Canine and Feline Coronavirus Infections—Genetic Outcomes and Vaccine Development." Veterinary Microbiology, vol. 169, no. 3-4, 2014, pp. 198–205.
5. Kipar, A., & Meli, M.L. "Feline Infectious Peritonitis: Still an Enigma?" Veterinary Pathology, vol. 51, no. 2, 2014, pp. 505–526.
6. Dickinson, P.J., et al. "Antiviral treatment of naturally occurring feline infectious peritonitis: Remdesivir and GS-441524." Frontiers in Veterinary Science, vol. 8, 2021, Article 653591.
7. Hartmann, K. "Feline Infectious Peritonitis." Veterinary Clinics: Small Animal Practice, vol. 35, no. 1, 2005, pp. 39–54.
8. Morris, D., et al. "Immunological Approaches to Feline Infectious Peritonitis." Veterinary Immunology and Immunopathology, vol. 209, 2019, pp. 49–54.
9. Addie, D.D., et al. "Feline coronavirus infection: ABCD guidelines on prevention and management." Journal of Feline Medicine and Surgery, vol. 21, no. 7, 2019, pp. 614–633.